Spinal fractures caused by trauma are usually easy to identify due to the amount of pain caused by the injury. Fractures are usually confirmed by XRAY, CT Scan or MRI scan.
An unstable fracture (ie one that can cause nerve damage or progressive deformity and pain) should be treated urgently with surgery or stabilisation. Most fractures however are stable and surgery is not necessarily required.
Vertebral fractures -deformations of the vertebral bodies that are observed in the X-ray of the spine and characterized according to their shape- are the most common manifestation of osteoporosis.
These fractures are usually identified clinically when the patient presents with back pain and in the radiograph of the spine an image is observed that is interpreted as a fracture of a vertebral body, more frequently in the thoracolumbar transition zone or in the centrotrophic region.
For osteoporotic vertebral compression fractures there are a number of options for treatment;
Pain management
Clinical vertebral fractures can cause severe pain that may even require hospitalization.
Non-steroidal anti-inflammatories, analgesics (including narcotic drugs and tramadol), transdermal lidocaine, and agents used to relieve neuropathic pain (eg, tricyclic antidepressants) are commonly used.
Although the pain of acute vertebral fracture usually disappears over several weeks, narcotics are often required temporarily to facilitate mobility and avoid prolonged bed rest.
Rehabilitation
Although its efficacy has not been fully demonstrated, the use of therapeutic exercise programs is recommended to reduce pain and improve strength, balance, functional status and quality of life. Back supports (ie, spinal orthoses) have been used in patients with acute vertebral fractures, but their benefits and harms have not been rigorously evaluated.
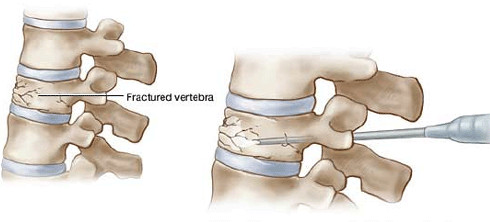
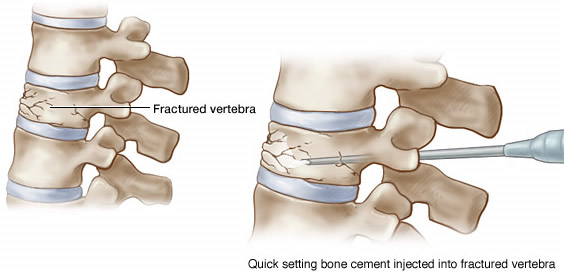
Vertebroplasty and kyphoplasty
Studies have reported the reduction of pain, disability and length of hospital stay among patients with an acute vertebral fracture who underwent these minimally invasive procedures, compared to those who did not.
Calcium and vitamin D
All current guidelines for the treatment of osteoporosis recommend an adequate intake of calcium (≥ 1,000 mg / day) and vitamin D (≥ 600 IU / day).
Pharmacotherapy
To reduce the risk of subsequent fractures in people with radiographic or clinical vertebral fractures not caused by a severe trauma or cancer, pharmacological treatment is indicated. Among the medications used are oral bisphosphonates (alendronate, ibandronate and risedronate), intravenous bisphosphonates (zoledronic acid), selective modulators of estrogen receptors (bazedoxifene, lasofoxifene and raloxifene), parathyroid hormone, denosumab, strontium ranelate and calcitonin, although the efficacy of the latter to reduce new vertebral fractures is questionable.